Speech Sound Disorders Explained: A parent's guide to Articulation, Phonological Disorders and Home Practice Strategies
- synapsekidsslp7
- Mar 2
- 10 min read
When a child begins to speak, every word is an experiment in sound and meaning. They begin to access language, shaping ideas into words long before their speech system can produce them with adult precision. Early mispronunciations like “wabbit” for rabbit or “tat” for cat are common and developmentally appropriate.
But speech development does not always follow the typical trajectory. When sound errors persist beyond expected ages or follow identifiable patterns, we enter the clinical domain of speech sound disorders (SSD). These disorders affect the production of speech sounds despite intact language comprehension and cognitive ability.
A speech sound disorder is defined as a communication condition in which a child has difficulty producing speech sounds accurately, consistently, or in alignment with developmental norms.According to the professional standards of the American Speech-Language-Hearing Association(ASHA), SSDs encompass problems with sound production, sound patterns, and the motor coordination required for speech.
SSD does not reflect intelligence or language comprehension. Many children with SSD understand complex ideas and use age-appropriate vocabulary but struggle to translate those ideas into conventional speech. This distinction shifts the clinical focus from assumptions about effort to the mechanics of sound production and motor learning.

Age of Sound Acquisition (Developmental Norms)
Speech development follows predictable ranges, not rigid deadlines. These milestones help clinicians determine whether errors reflect typical development or disorder.
Sound | Expected Mastery Age |
/p, b,m/ | 3 years |
/t, d, n/ | 3 years |
/k,g/ | 4 years |
/f,v/ | 4 years |
/s,z/ | 5 years |
/l/ | 5 years |
/r/ , /th/ | 6-7 years |
Errors beyond these ranges may warrant evaluation, particularly if intelligibility is reduced or patterns persist.

What Are Speech Sound Disorders?
SSD encompasses several categories:
Articulation Disorders
An articulation disorder involves difficulty producing specific speech sounds due to challenges with motor placement or execution. Children with articulation disorders generally understand the sound they intend to produce but struggle to position the tongue, lips, or jaw correctly to create the target sound.
Articulation disorders often due to one of the following types of errors (SODA) that reduce intelligibility:
S: Substitution (e.g., "wion" for "lion")
O: Omission (e.g., "poon" for "spoon")
D: Distortion (e.g., slushy "s" rather clear "s". distortions are common for airflow sounds)
A: Addition (e.g., "balue" for "blue")

Characteristics of Articulation Disorders
Articulation disorders typically present with:
Errors limited to one or a few specific sounds
Consistent misproduction of those sounds
Placement-based difficulty (tongue, lip, or jaw positioning)
No broader pattern affecting multiple sound groups
Intact understanding of speech and language concepts
For example:
/r/ → /w/ (“wabbit”)
Lisp on /s/ (tongue placement between teeth)
Distorted /l/ (inadequate tongue elevation)
To understand articulation disorders, it helps to understand how speech sounds are classified by place and manner of articulation.
Place of Articulation (Where the Sound Is Made)
Place | Description | Example Sounds |
Bilabial | Lips together | /p, b, m/ |
Labiodental | Lip + teeth | /f, v/ |
Alveolar | Tongue to ridge behind teeth | /t, d, s, z, n, l/ |
Palatal | Tongue to hard palate | /ʃ (sh), tʃ (ch)/ |
Velar | Back of tongue to soft palate | /k, g/ |
Dental | Tongue between teeth | /th/ |
Manner of Articulation (How the Sound Is Made)
Manner | Description | Example Sounds |
Stop | Air briefly blocked | /p, b, t, d, k, g/ |
Fricative | Continuous airflow | /f, s, v, z, sh, th/ |
Affricate | Stop + fricative | /ch, j/ |
Nasal | Air through nose | /m, n/ |
Liquid | Smooth airflow | /l, r/ |
Glide | Quick transition | /w, y/ |

Treatment Principles
Evidence-based speech therapy for articulation disorder often follows motor learning principles:
Teach correct placement (tongue and lip positioning)
Use hierarchical practice (sound → syllable → word → phrase → sentence): This is often reflected in the home practice sheets provided by your speech therapist
Provide high repetition for motor memory
Gradually fade cues as accuracy improves
Generalize skills to conversation
Phonological Disorder (With Phonological Processes Explained)
A phonological disorder involves difficulty organizing the sound system and applying age-appropriate sound patterns. Unlike articulation disorders (which focus on individual sound placement), phonological disorders reflect rule-based errors that affect groups of sounds.
Children with phonological disorders use developmental simplifications beyond the age when those patterns typically resolve. These patterns known as phonological processes are normal in early speech development but should diminish as the child’s sound system matures.
What Are Phonological Processes?
Phonological processes are systematic patterns children use to simplify speech as they learn the sound system. For example, young children may omit ending sounds or simplify clusters because their motor and linguistic systems are still developing.
These processes are expected in early childhood. Persistence beyond developmental norms suggests a phonological disorder.
Common processes include:
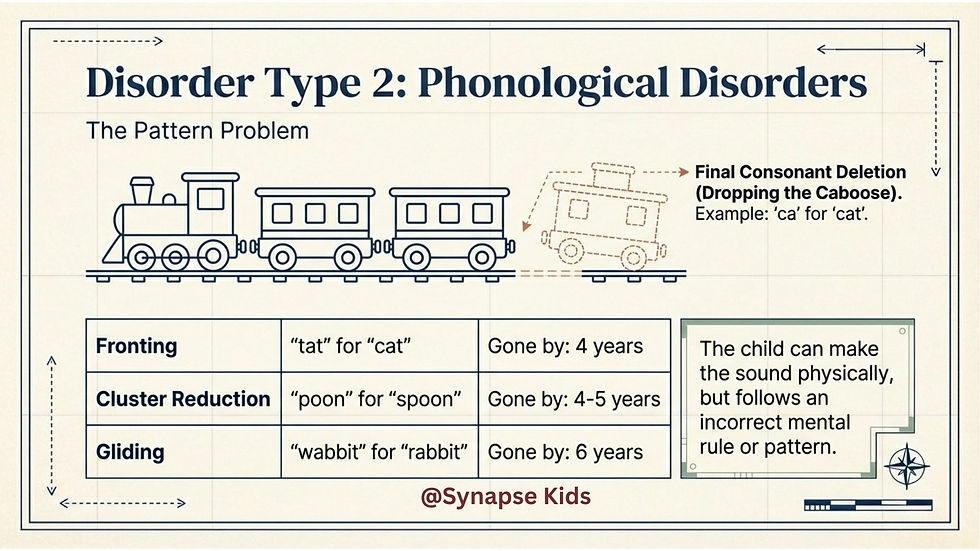
Phonological Process | Description | Example | Expected Elimination |
Final consonant deletion | Omitting the ending sound | “ca” → cat | 3 years |
Fronting | Substituting a front sound for a back sound | “tat” → cat | 4 years |
Cluster reduction | Simplifying consonant clusters | “poon” → spoon | 4–5 years |
Gliding | Replacing /r/ or /l/ with /w/ | “wabbit” → rabbit | 6 years |
When Processes Become a Disorder
Phonological processes are part of normal development in young children. A disorder is considered when:
Processes persist beyond expected ages
Multiple sound patterns are affected
Intelligibility is reduced
Errors follow predictable patterns rather than isolated articulation difficulties
For example, a 5-year-old who still deletes final consonants (“ca” for cat) may require intervention because this process should have resolved earlier.
Treatment Approaches for Phonological Disorders
Phonological therapy targets the sound system and rule-based patterns rather than individual sound placement. The goal is to help the child learn the organization of sounds so that speech becomes more intelligible and developmentally appropriate.
Unlike articulation therapy which teaches motor placement for specific sounds, phonological therapy addresses systemic patterns such as final consonant deletion or cluster reduction. Treatment shifts the focus from single sounds to the structure of the sound system. Speech therapists often use of these approaches to treat phonological process disorders
Minimal Pairs Approach (Pattern Contrast)
The minimal pairs approach uses word pairs that differ by only one sound to highlight how sound changes alter meaning.
Example minimal pair:
“cat” vs “tat”
Here the contrast demonstrates that substituting /t/ for /k/ changes meaning. The child learns that small sound differences matter for communication.
Cycles Approach (Pattern Rotation)
The cycles approach treats phonological patterns in rotating cycles rather than mastering one sound before moving to the next.
For example, a therapy cycle might target:
Final consonants
Cluster reduction
Fronting
Each cycle revisits patterns systematically, allowing gradual improvement over time.
Caboose metaphor: Imagine speech as a train. Final consonants are like the caboose, the last car of the train. In final consonant deletion, the child drops the caboose, saying “ca” instead of “cat.” Cycles therapy teaches the child to keep the entire train intact, gradually reinforcing the pattern of ending sounds.
Complexity Approach (Advanced Pattern Targeting)
The complexity approach targets more complex sounds or structures to promote broader system change.
For example, teaching clusters like “sp” or “st” may improve simpler sound patterns as a byproduct of learning complex structures.
Childhood Apraxia of Speech (CAS)
Childhood apraxia of speech (CAS) is a pediatric motor speech disorder characterized by impaired planning and programming of movement sequences necessary for accurate speech production.
Unlike articulation disorders (motor execution) or phonological disorders (sound system organization), CAS reflects difficulty generating and sequencing motor plans for speech. The child knows what they want to say, and the muscles are not weak, but the brain has difficulty coordinating the precise, rapid movements required for intelligible speech.
According to ASHA, CAS is defined by deficits in the precision and consistency of movements underlying speech in the absence of neuromuscular deficits.
Core Characteristics of CAS
CAS is diagnosed based on a constellation of features rather than a single marker. Three widely recognized characteristics include:
Inconsistent errors on consonants and vowels
Lengthened or disrupted coarticulatory transitions between sounds
Inappropriate prosody (abnormal rhythm, stress, or intonation)
Additional clinical markers may include:
Groping behaviors (visible searching for placement)
Vowel distortions
Greater difficulty with longer or more complex words
Limited sound inventory in early speech
Reduced intelligibility disproportionate to age
A key distinguishing feature is inconsistency. A child may produce the same word differently across attempts because the motor plan is unstable.
Clinical Distinction From Other SSDs
CAS | Articulation Disorder | Phonological Disorder |
Motor planning deficit | Motor placement deficit | Rule-based sound system deficit |
Inconsistent errors | Consistent errors | Pattern-based errors |
Prosody differences | Typical prosody | Typical prosody |
Difficulty sequencing | Difficulty placing | Difficulty organizing |
Treatment Principles for CAS
CAS therapy is motor-based and grounded in motor learning theory. Because the difficulty lies in planning movement sequences, therapy emphasizes:
High-frequency, structured repetition
Dynamic cueing (visual, tactile, auditory)
Gradual fading of support
Practice of movement sequences, not isolated sounds
Functional word targets
Evidence-based approaches often include dynamic temporal and tactile cueing (DTTC) and other intensive motor planning frameworks.
Unlike articulation therapy, CAS treatment does not rely on traditional sound hierarchies alone. Instead, it focuses on:
Syllable shapes
Movement transitions
Increasing length and complexity gradually
Frequency matters. Children with CAS often benefit from more intensive therapy schedules to build motor memory.
Dysarthria
Dysarthria is a motor speech disorder resulting from neuromuscular impairment affecting the strength, speed, coordination, or tone of the speech musculature.
Unlike CAS, dysarthria involves deficits in motor execution rather than planning. The brain generates the correct motor plan, but the muscles cannot execute the plan efficiently due to weakness, incoordination, or abnormal tone.
According to ASHA, dysarthria is characterized by speech disturbances resulting from impaired muscular control of the speech mechanism.
Causes of Dysarthria
Dysarthria may be associated with:
Neurological conditions
Cerebral palsy
Traumatic brain injury
Genetic or neuromuscular disorders
Developmental motor disorders
The specific presentation depends on the underlying neurological involvement.
Speech Characteristics of Dysarthria
Children with dysarthria may demonstrate:
Slurred or imprecise articulation
Reduced speech volume
Breathiness
Monotone prosody
Slow or effortful speech
Reduced breath support
Hypernasality
Errors are typically consistent because the underlying weakness or coordination difficulty is stable.
Treatment Principles for Dysarthria
Therapy for dysarthria focuses on improving functional intelligibility by targeting the physiological components of speech:
Breath support training
Rate control strategies
Over-articulation techniques
Prosody support
Strength and coordination exercises (functional, speech-based)
Treatment is tailored to the child’s specific neuromuscular profile.

Intelligibility: Why It Matters
Intelligibility refers to how well unfamiliar listeners understand a child’s speech.
General guidelines:
Age | Expected Intelligibility |
2 years | ~50% |
3 years | ~75% |
4 years | 90–100% |
Reduced intelligibility can affect social interaction and academic participation. Evaluation helps determine underlying causes and appropriate intervention.
Orofacial Myofunctional Considerations in Speech Sound Therapy
Traditional articulation therapy focuses on teaching accurate sound placement and motor practice (e.g., where to put the tongue for /s/ or /r/). However, when structural or functional differences are present; such as tongue thrust, low tongue resting posture, mouth breathing, or limited lingual mobility progress may plateau without addressing the underlying myofunctional patterns.
Orofacial myofunctional therapy (OMT) targets the resting posture and functional patterns of the lips, tongue, and jaw. For example:
A child with an interdental /s/ may also have a forward tongue resting posture.
A persistent open-mouth posture may impact bilabial strength and stability.
Limited tongue elevation can affect alveolar and palatal sounds.
While traditional articulation therapy drills correct sound production in structured contexts, OMT works on:
Establishing nasal breathing
Normalizing tongue-to-palate resting posture
Lip seal and jaw stability
Coordinated swallow patterns
The key difference:Articulation therapy treats the symptom (sound error).Orofacial myofunctional therapy addresses the underlying muscular pattern that may be contributing to the error.
When integrated appropriately, combining motor-based articulation practice with foundational myofunctional support can lead to more stable, generalized speech outcomes.
How to Help Your Child Practice Sounds at Home
(Parent-Friendly, Placement-Focused Guide)
Before we talk about tricks and tools, here’s the most important thing to understand:
Speech sounds are made by very specific movements of the tongue, lips, jaw, and airflow. When a child can’t produce a sound, it’s usually not about effort, it’s about not knowing where their tongue should go.
Your job at home isn’t to “correct” constantly. It’s to gently guide placement and make practice playful.
Let’s walk through a few of the most common sounds parents ask about.
Animal Metaphor | Sound | Placement Cues | Parent Script | Common Errors | Practice Tip |
🐱 Coughing Cat | /k/, /g/ | Tongue lifts in the back and touches the soft palate (velum). Lips stay relaxed. Short burst of air. | “Let’s be a coughing cat. Say ‘kuh’ like a tiny cough.” | “tat” for cat / “do” for go (fronting) | Use a tongue depressor or spoon to gently guide the front of the tongue down (light pressure only). A lollipop placed toward the back of the tongue can cue elevation. Lying down may help gravity guide the tongue backward. |
🐘 Lifting Elephant | /l/ | Tongue tip lifts to the alveolar ridge (bumpy spot behind top teeth). Air flows around the sides. | “Lift your elephant trunk to the spot behind your teeth.” | “wove” for love / “yike” for like | Try the Cheerio trick: place a Cheerio on the ridge and have the child “hold it with your tongue.” For /t/ and /d/, tap the Cheerio and let it pop off. For /l/, hold it and let air flow. |
🐍 Hissing Snake | /s/ | Teeth together. Tongue behind teeth (not between). Steady airflow. | “Be a snake in a cage. Keep your tongue "snake" behind the cage.” | Lisp (tongue between teeth) | Use the up-and-down arm strategy: child runs finger down your arm while saying “ssssss” to lengthen airflow and control duration. Keep it smooth and steady. |
🦏 Poking Rhino | /th/ | Tongue tip gently peeks between teeth. Soft airflow. No biting. | “Let your rhino horn poke out just a tiny bit.” | Substitution with /f/ or /d/ | Use a mirror so the child can see the tongue peek. Gentle air only — it should feel soft, not forceful. |
🐰 Bunny Teeth | /f/ | Top teeth rest on bottom lip. Air blows out. | “Make bunny teeth. Teeth on lip and blow.” | Substitution with /p/ or /b/ (air blocked)or with /th/ | Lightly tap the bottom lip to remind placement. The air should feel like a gentle breeze. |
🦁 Roaring Lion | /r/ | Tongue pulls back and slightly up (bunched) or curls up (retroflex) (not touching teeth or roof). Lips may be slightly rounded. Strong, voiced sound. tight tongue muscle | “Growl like a lion: rrrr.” | “wabbit” for rabbit / weak or gliding /r/ | /r/ is motorically complex. Encourage tongue retraction (back movement) and avoid overemphasizing tongue-tip placement. Many children need time and structured practice for this sound. |

Online Resources & Apps for Home Speech Practice
When it comes to mastering speech sounds at home, combining printable sheets, interactive apps, and structured games is often most effective. Below are a few tools that parents can use right away with free options or free content.
APP: Articulation Station / Articulation Station Hive
Best for: Structured articulation practice for specific sounds
Games: Pink Cat Games (Speech Therapy Games)
Best for: Game-based repetition
Website: www.mommyspeechtherapy.com
Best for : free practice lists by sounds
If you’re reading this and still wondering whether your child’s speech is “just a phase” or something more, trust that instinct. Speech development follows patterns, but it is not one-size-fits-all. The earlier we identify whether a sound error is developmental, phonological, or motor-based, the easier and more efficient therapy can be. An evaluation doesn’t commit you to therapy, it gives you clarity. And clarity brings relief. If you’re unsure, overwhelmed, or simply want expert guidance, scheduling an evaluation is a proactive step toward confident communication for your child. When in doubt, get answers. Early support makes all the difference.


Comments